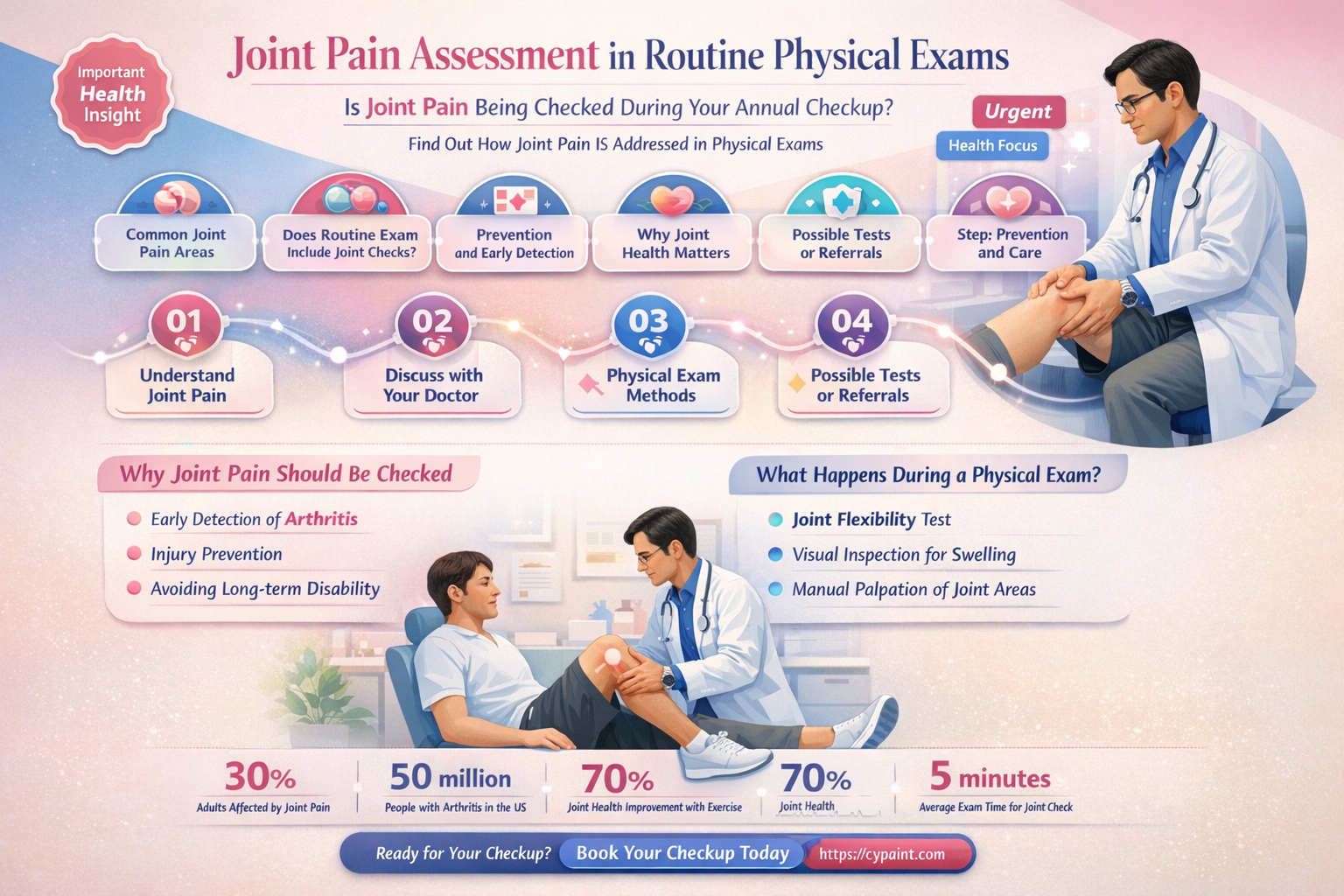
Joint pain is a common concern that often prompts individuals to seek medical evaluation, and understanding whether it is assessed during a physical exam is essential for both patients and healthcare providers. A physical exam is a comprehensive evaluation of a patient’s overall health, during which a healthcare professional examines various body systems, including the musculoskeletal system. Joint pain is indeed a critical component of this assessment, as it can indicate underlying conditions such as arthritis, injury, infection, or systemic diseases. During the exam, the provider may inspect the affected joints for swelling, redness, or deformity, test their range of motion, and apply pressure to identify tenderness or discomfort. Additionally, the exam may include neurological and vascular assessments to rule out related issues. While joint pain is a significant part of a physical exam, further diagnostic tests like imaging or blood work may be necessary to determine the exact cause and guide appropriate treatment.
| Characteristics | Values |
|---|---|
| Joint Pain Assessment | Yes, joint pain is a common component of a physical exam, especially in musculoskeletal evaluations. |
| Purpose | To identify underlying conditions such as arthritis, injury, infection, or systemic diseases. |
| Methods | Inspection, palpation, range of motion testing, and assessment of swelling, redness, warmth, and tenderness. |
| Associated Symptoms Evaluated | Stiffness, swelling, deformity, and functional limitations. |
| Relevant Medical History | Duration, onset, aggravating/alleviating factors, and associated symptoms (e.g., fever, weight loss). |
| Diagnostic Tools | May include imaging (X-rays, MRI), blood tests (ESR, CRP), or joint fluid analysis. |
| Common Conditions Identified | Osteoarthritis, rheumatoid arthritis, gout, lupus, infections (e.g., septic arthritis). |
| Referral Criteria | Severe pain, systemic symptoms, or suspected serious conditions may require specialist referral. |
| Documentation | Detailed notes on joint appearance, pain location, intensity, and impact on daily activities. |
| Follow-Up | Monitoring for progression, response to treatment, and need for further interventions. |
Explore related products

$16.99 $37.95





What You'll Learn
![]()
Joint Inspection Techniques
Joint inspection is a critical component of the musculoskeletal assessment during a physical exam, particularly when evaluating joint pain or dysfunction. The process involves a systematic approach to identify abnormalities, assess range of motion, and determine the underlying cause of symptoms. Inspection begins with visual observation of the joint for swelling, deformity, erythema, or asymmetry compared to the contralateral joint. The examiner should note any visible signs of inflammation, such as warmth or redness, which may indicate conditions like arthritis or infection. This initial step provides valuable clues about the joint’s condition before proceeding to more hands-on techniques.
Palpation is the next essential technique, where the examiner uses their hands to assess joint tenderness, temperature, and the presence of effusions or bony abnormalities. Gentle pressure is applied around the joint to identify areas of maximal tenderness, which can localize the source of pain. For example, tenderness over the joint line may suggest meniscal injury in the knee, while tenderness over the epicondyles could indicate tendinitis. Palpation also helps detect joint instability or crepitus, a grinding sensation that often signifies degenerative changes. The examiner should use a systematic approach, palpating both the affected and unaffected joints for comparison.
Range of motion (ROM) testing is another cornerstone of joint inspection. Active and passive ROM assessments help differentiate between pain originating from the joint itself and pain caused by surrounding structures, such as muscles or tendons. The examiner guides the patient through full flexion and extension, noting any limitations, pain, or abnormal movements. For instance, a reduced ROM with pain at the end range may suggest a mechanical block, while pain throughout the range could indicate inflammation. Special tests, like the McMurray test for meniscal tears or the Lachman test for ACL integrity, may be incorporated based on the suspected pathology.
Assessment of joint stability is crucial, especially in weight-bearing joints like the knee or ankle. Techniques such as varus/valgus stress tests or anterior/posterior drawer tests help evaluate ligamentous integrity. Instability may indicate acute trauma or chronic laxity, guiding further diagnostic or treatment decisions. Additionally, gait analysis provides dynamic information about joint function. Observing the patient’s walk can reveal abnormalities like limping, antalgic gait, or joint misalignment, which may not be apparent during static examination.
Finally, specialized techniques such as assessing for crepitus, effusions, or joint locking are tailored to specific joints. For example, the elbow may be evaluated for olecranon bursitis by palpating for swelling posteriorly, while the shoulder may require tests like the impingement sign for rotator cuff pathology. Documentation of findings should be detailed, including the location, quality, and severity of symptoms, as well as any observed abnormalities during inspection, palpation, and movement. Mastery of these joint inspection techniques ensures a comprehensive assessment, enabling accurate diagnosis and appropriate management of joint-related conditions.
Ink or Paint First? The Great Art Debate
You may want to see also
Explore related products






![]()
Pain Assessment Methods
Pain assessment is a critical component of any physical examination, particularly when evaluating joint pain. The first method commonly employed is the verbal self-report, where patients describe the location, intensity, duration, and quality of their pain. Clinicians often use standardized pain scales, such as the Numerical Rating Scale (NRS) or the Visual Analog Scale (VAS), to quantify pain intensity. For joint pain, patients may be asked to specify whether the pain is sharp, dull, throbbing, or radiating, which helps in diagnosing the underlying cause. This method is direct and patient-centered, ensuring that the individual’s experience is accurately captured.
Physical examination techniques play a pivotal role in assessing joint pain. Inspection, palpation, and range-of-motion testing are standard procedures. During inspection, the clinician observes for swelling, redness, deformity, or asymmetry in the joint. Palpation involves gently pressing around the joint to identify tenderness, warmth, or effusion, which can indicate inflammation or injury. Range-of-motion tests assess how freely the joint moves, with restricted movement often suggesting pain or structural issues. These methods provide objective findings that complement the patient’s subjective reports.
Functional assessment is another important tool in evaluating joint pain. Clinicians may ask patients to perform specific movements or activities that typically exacerbate pain, such as walking, squatting, or lifting. Observing how pain affects the patient’s ability to function provides insights into its severity and impact on daily life. For example, a patient with knee pain may struggle with stair climbing, indicating significant impairment. This approach bridges the gap between clinical findings and real-world consequences of joint pain.
In addition to these methods, diagnostic imaging and laboratory tests may be utilized to further assess joint pain. X-rays, MRI, or ultrasound can reveal structural abnormalities like fractures, arthritis, or soft tissue damage. Blood tests, such as inflammatory markers (e.g., ESR, CRP), may help identify conditions like rheumatoid arthritis or gout. While these tests are not part of the physical exam itself, they are often ordered based on findings from the initial assessment and are crucial for confirming diagnoses.
Lastly, pain behavior observation is an indirect but valuable method. Clinicians may note nonverbal cues such as grimacing, guarding, or reluctance to move certain joints, which can indicate pain even if the patient underreports it. This method is particularly useful in patients who have difficulty communicating, such as children or those with language barriers. Combining these assessment methods ensures a comprehensive evaluation of joint pain, enabling accurate diagnosis and tailored treatment plans.
In conclusion, joint pain assessment in a physical exam involves a multifaceted approach, including verbal self-reports, physical examination techniques, functional assessments, diagnostic tools, and observational methods. Each method contributes unique insights, ensuring that the clinician can address the pain’s cause, severity, and impact effectively.
The Scream Mask: Inspired by Edvard Munch's Painting?
You may want to see also
Explore related products





![]()
Range of Motion Testing
Range of Motion (ROM) testing is a critical component of a physical examination, particularly when assessing joint pain or dysfunction. This assessment helps healthcare providers evaluate the flexibility, mobility, and overall health of a patient’s joints. During ROM testing, the examiner measures the degree of movement around a specific joint, both actively (patient-initiated) and passively (examiner-assisted). This distinction is important because limitations in active ROM may indicate muscle weakness or pain, while restrictions in passive ROM often suggest structural issues, such as joint stiffness or inflammation. ROM testing is essential for diagnosing conditions like arthritis, injuries, or post-surgical recovery, as it provides objective data about joint function.
To perform ROM testing, the examiner typically uses a goniometer, a tool designed to measure joint angles accurately. The process begins with the patient in a comfortable position, and the joint is moved through its full range of motion. For example, in testing knee flexion, the patient lies supine, and the examiner gently bends the knee while keeping the thigh stable. The goniometer is aligned with the joint’s axis of motion, and the maximum angle achieved is recorded. Both active and passive ROM are measured for comparison. It’s crucial to assess both sides of the body (e.g., both knees) to identify asymmetries, which can highlight abnormalities.
ROM testing is not limited to large joints like the knee or shoulder; it also applies to smaller joints such as the fingers, wrists, and ankles. Each joint has a normal range of motion based on anatomical standards, and deviations from these norms can indicate pathology. For instance, reduced wrist extension might suggest tendonitis, while limited shoulder abduction could point to a rotator cuff injury. The examiner must also observe for pain, crepitus (grinding or cracking sounds), or instability during movement, as these findings provide additional clinical context.
Incorporating ROM testing into a physical exam requires a systematic approach. The examiner should start with visual inspection, noting any swelling, deformity, or misalignment. Palpation follows to assess tenderness, warmth, or effusion around the joint. Finally, ROM testing is conducted, ensuring the patient is relaxed to avoid muscle guarding, which can falsely limit motion. Clear communication with the patient is essential, as they should indicate when pain or resistance is felt during the assessment.
ROM testing is invaluable for monitoring progress in patients with joint pain or injuries. For example, after a knee surgery, regular ROM measurements help track recovery and guide rehabilitation. It also assists in differentiating between musculoskeletal and neurological causes of limited mobility. By integrating ROM testing into the physical exam, healthcare providers can make informed decisions about treatment plans, whether they involve physical therapy, medication, or surgical intervention. In summary, ROM testing is a fundamental tool for evaluating joint health and addressing pain as part of a comprehensive physical examination.
Touch Up Your RV: Las Vegas Paint Guide
You may want to see also
Explore related products






![]()
Swelling and Redness Evaluation
During a physical examination, the evaluation of swelling and redness in joints is a critical component, especially when assessing joint pain. This process involves a systematic approach to identify and quantify these symptoms, which can provide valuable insights into the underlying condition. The examiner begins by visually inspecting the joint for any noticeable swelling, comparing it to the contralateral joint or a known normal state. Swelling, or edema, is often indicative of inflammation, fluid accumulation, or tissue damage within the joint. Redness, on the other hand, is typically assessed by examining the overlying skin for erythema, which may suggest increased blood flow or inflammation in the area. Both swelling and redness are key indicators of joint pathology and are essential in diagnosing conditions such as arthritis, infection, or injury.
To perform a thorough swelling evaluation, the examiner should use both visual and tactile methods. Palpation allows the clinician to determine the consistency, temperature, and tenderness of the swollen area. For instance, pitting edema, where an indentation remains after pressure is applied, may indicate fluid retention, whereas non-pitting edema could suggest more chronic inflammatory changes. The degree of swelling can be measured using a tape measure or by comparing the circumference of the affected joint to the unaffected one. Documenting the exact location, size, and characteristics of the swelling is crucial for monitoring progression or response to treatment.
Redness evaluation requires careful observation under adequate lighting. The examiner should note the extent, intensity, and distribution of erythema around the joint. It is important to differentiate between redness caused by increased blood flow (hyperemia) and that resulting from inflammation or infection. Associated symptoms such as warmth, pain, or tenderness upon palpation can further guide the diagnosis. For example, a warm, red, and swollen joint may raise suspicion for septic arthritis, whereas redness without warmth could be more consistent with a systemic inflammatory condition like rheumatoid arthritis.
Incorporating swelling and redness evaluation into the physical exam involves a structured approach. The examiner should first gather a detailed history, including the onset, duration, and aggravating factors of the joint pain. This information helps in focusing the examination and interpreting the findings accurately. During the assessment, the clinician should systematically inspect and palpate the joint, noting any deviations from normal. Additional maneuvers, such as assessing range of motion or performing specific provocative tests, can complement the evaluation by identifying functional limitations associated with the swelling and redness.
Finally, the findings from the swelling and redness evaluation should be integrated with other clinical data to formulate a differential diagnosis. For instance, acute onset of severe swelling, redness, and pain in a single joint may point toward gout or septic arthritis, whereas symmetric involvement with morning stiffness could suggest rheumatoid arthritis. Imaging studies or laboratory tests may be ordered to confirm the diagnosis, but the initial physical exam, including the assessment of swelling and redness, remains a cornerstone in guiding further management. By meticulously evaluating these signs, healthcare providers can ensure a comprehensive and accurate approach to patient care.
Understanding the Difference: 1K and 2K Paints
You may want to see also
Explore related products






![]()
Joint Tenderness Examination
During the joint tenderness examination, specific joints are targeted based on the patient’s symptoms or clinical suspicion. Commonly assessed joints include the knees, shoulders, wrists, and small joints of the hands and feet. For example, in a patient with suspected rheumatoid arthritis, the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints are carefully palpated for tenderness, as these are frequently involved. The examiner must be methodical, ensuring all relevant areas are covered while avoiding excessive pressure that could cause unnecessary pain. Documenting the exact location and intensity of tenderness is essential for diagnosis and monitoring disease progression.
Proper patient positioning is crucial for an accurate joint tenderness examination. The joint should be in a relaxed, neutral position to minimize muscle tension and allow for precise palpation. For instance, when examining the knee, the patient may be positioned supine with the knee slightly flexed. Clear communication with the patient is vital; the examiner should instruct the patient to indicate when they feel tenderness and describe its nature (e.g., sharp, dull, or throbbing). This feedback helps the examiner correlate tenderness with specific structures within the joint, such as the synovium, capsule, or periarticular tissues.
Interpreting the findings of a joint tenderness examination requires clinical context. Localized tenderness often suggests an inflammatory or traumatic process, while diffuse tenderness may indicate a systemic condition or fibromyalgia. For example, tenderness over the joint line of the knee could point to meniscal injury, whereas tenderness over the patellar tendon might suggest tendinitis. Comparing findings between bilateral joints can also be informative, highlighting asymmetry that may indicate unilateral pathology. The examiner should integrate these findings with other components of the physical exam, such as range of motion and gait analysis, to form a comprehensive assessment.
In conclusion, joint tenderness examination is a fundamental skill in the physical assessment of patients with joint pain. It requires a structured approach, combining inspection, palpation, and patient feedback to identify areas of tenderness accurately. By localizing and characterizing tenderness, clinicians can narrow down potential diagnoses and guide further diagnostic or therapeutic interventions. Mastery of this technique enhances the ability to differentiate between various musculoskeletal conditions, ensuring targeted and effective patient care.
Painting a 1973 Corvette: How Much Does It Cost?
You may want to see also
Frequently asked questions
Yes, joint pain assessment is often included in a routine physical exam, especially if the patient reports discomfort or if there are visible signs of inflammation or deformity.
Physicians typically use palpation, range of motion tests, and visual inspection to evaluate joint pain, swelling, tenderness, and mobility during a physical exam.
No, while a physical exam provides valuable information, additional tests like X-rays, blood work, or imaging studies may be needed for a definitive diagnosis.
Conditions such as arthritis, bursitis, tendinitis, gout, or injuries like sprains and fractures can often be identified or suspected during a physical exam.
Yes, always mention any joint pain, even if mild, as it could be an early sign of an underlying condition that requires further evaluation or treatment.